NAFLD vs. NASH: Understanding the Fatty Liver Spectrum and Fibrosis Risks
Imagine waking up from your morning coffee routine to read a lab report stating you have fat accumulating in your liver. It sounds alarming, but before the panic sets in, you need to understand exactly what is happening inside your body. For decades, doctors and patients alike struggled to distinguish between simple fatty liver and the aggressive form that can actually damage the organ. The distinction between Non-Alcoholic Fatty Liver Disease (NAFLD), which serves as an umbrella term, and Non-Alcoholic Steatohepatitis (NASH), its more severe manifestation, is critical for your long-term health outlook.
This isn't just academic jargon; it dictates your risk of developing cirrhosis and whether you need aggressive medical intervention or just lifestyle tweaks. Recent updates in terminology suggest we might call it MASLD soon, but the underlying biology remains the same. We're going to break down how these conditions differ, what happens when scarring begins, and why modern medicine finally has treatments ready for those who need them.
The Core Difference Between Simple Fat and Inflammation
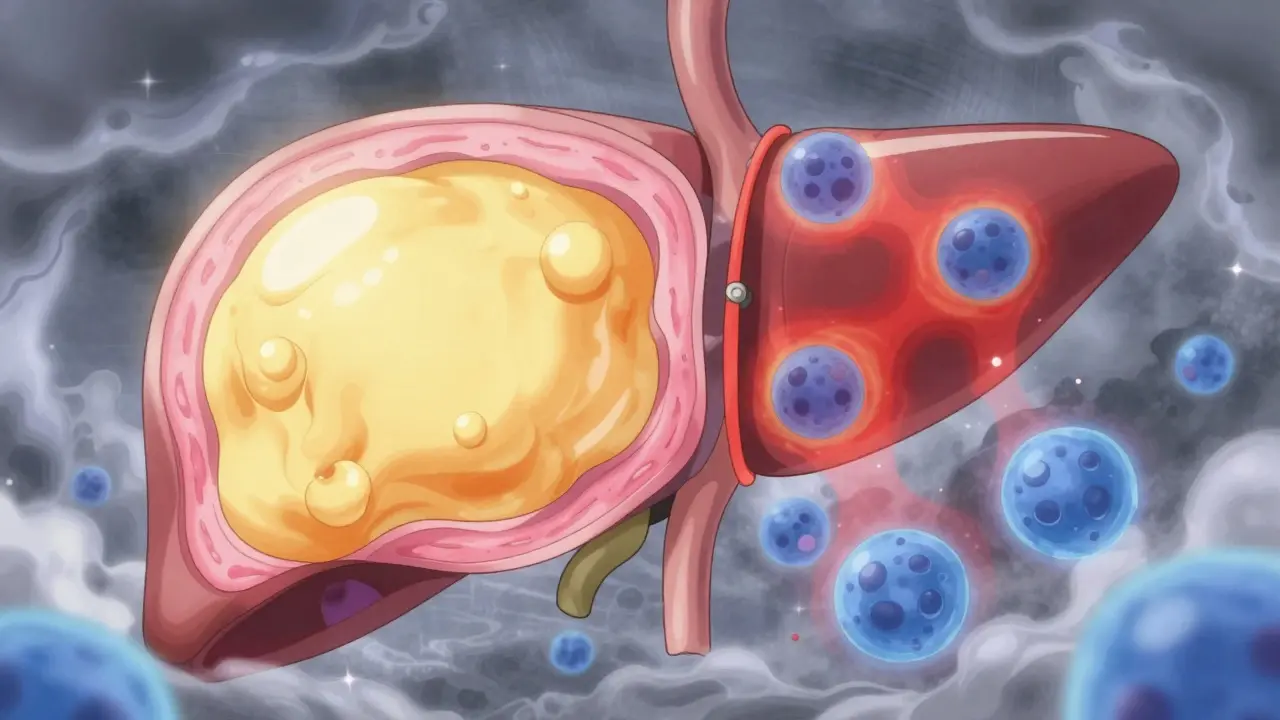
When people first get diagnosed, they often hear the term "fatty liver." While common, this label hides a crucial detail: not all fatty livers act the same way. Think of your liver like a hardworking employee. Sometimes, it gets a little overweight due to excess calories, much like gaining weight yourself, but it keeps functioning normally. This state is often referred to as Non-Alcoholic Fatty Liver (NAFL). Here, there is significant fat accumulation-specifically 5% or greater of the liver tissue-but no injury to the cells.
NASH represents a different scenario entirely. In this condition, that fat triggers inflammation and direct damage to the liver cells themselves. Medical professionals look for signs called hepatocyte ballooning, where cells swell under stress, and lobular inflammation. According to guidelines from the American Association for the Study of Liver Diseases, simply having fat isn't enough to diagnose NASH; there must be evidence of cellular injury.
Why does this matter? Because NAFL typically follows an indolent course. Many patients live with simple steatosis for years without their liver function deteriorating significantly. However, once inflammation kicks in with NASH, the game changes. A 2019 longitudinal study published in Hepatology tracked over 1,200 patients for 15 years. They found that only 12.3% of those with simple NAFL developed significant scarring, whereas nearly half of the NASH group progressed to fibrosis. That gap determines whether you can manage this with diet alone or if you require closer monitoring and medication.
| Feature | Non-Alcoholic Fatty Liver (NAFL) | Non-Alcoholic Steatohepatitis (NASH) |
|---|---|---|
| Fat Accumulation | Present (>5%) | Present (>5%) |
| Inflammation | Absent or Minimal | Present |
| Cell Injury | No | Yes (Ballooning) |
| Risk of Fibrosis | Low (Approx. 12% over 15 years) | High (Approx. 42% over 15 years) |
| Progression Risk | Stable | Can advance to Cirrhosis |
The Silent Danger: Fibrosis Staging
Whether you have NAFL or NASH, the metric that truly predicts your health outcome is fibrosis. You can think of fibrosis as scar tissue forming on the liver. When the liver repairs itself after repeated injury, it lays down collagen scars instead of healthy tissue. These scars do not work. As they multiply, they stiffen the organ, leading to reduced function.
Doctors stage this scarring on a scale from 0 to 4. Stage 0 means no visible fibrosis. Stage 1 involves mild scarring around the blood vessels. Stage 2 indicates more widespread scarring, while Stage 3 shows bridging fibrosis connecting major areas. Once you reach Stage 4, the condition has evolved into cirrhosis, which is permanent liver hardening.
Experts emphasize that fibrosis stage, not just the diagnosis of NASH, is the strongest predictor of mortality. According to data from the European Association for the Study of the Liver registry, patients with advanced fibrosis (Stage 3 or 4) face a 10-year liver-related mortality rate of up to 25%, compared to less than 2% for those with early-stage or no fibrosis. This reality is why identifying high-risk individuals through non-invasive scoring is so vital before irreversible damage occurs.
Navigating Diagnosis in 2026
If your primary care physician notices elevated liver enzymes, specifically ALT and AST during a routine blood test, the investigation begins. Normal ALT levels generally fall between 7 and 55 U/L. If yours reads higher, especially alongside a history of metabolic syndrome, you might be flagged for further testing. However, blood tests alone cannot definitively distinguish between simple fat and inflammation.
To dig deeper, clinicians calculate the FIB-4 score. This formula takes your age, platelet count, ALT, and AST into account. A score above 1.30 suggests possible advanced fibrosis, while scores exceeding 2.67 indicate a high probability. For those whose numbers are borderline, the next step often involves ultrasound or MRI-PDFF. Ultrasound can detect fat accumulation once it reaches about 20-30% of the liver volume, offering a quick visual confirmation of steatosis.
For more precise quantification of fat and stiffness, Elastography, commonly known as FibroScan, is the preferred tool in many clinics. It measures liver stiffness in kilopascals (kPa); a reading over 7.1 kPa often flags significant fibrosis. Despite the availability of these technologies, only a liver biopsy provides 100% specificity for diagnosing NASH. Yet, biopsies are invasive. There is a small risk of serious complications (about 0.01% to 0.1%), so guidelines recommend them only when non-invasive tests strongly suspect advanced disease or when planning specific drug therapies.
The Shift to New Terminology: MASLD and MASH
You may notice doctors starting to use different terms lately. In June 2023, major international liver societies agreed that "Non-Alcoholic" was potentially stigmatizing and inaccurate since small amounts of alcohol do not disqualify a person from having a metabolic liver condition. Consequently, they introduced Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD).
This new classification removes the focus on abstinence from alcohol and focuses squarely on the metabolic drivers. To meet the criteria for MASLD, a patient needs fat in the liver plus one additional metabolic health issue, such as overweight status, type 2 diabetes, or hypertension. The severe inflammatory version is now termed Metabolic Dysfunction-Associated Steatohepatitis (MASH).
This change isn't just semantics; it helps broaden eligibility for screening and treatment. It acknowledges that the root cause is often metabolic dysfunction-how your body processes sugar and fat-rather than just avoiding alcohol. This alignment ensures that patients with metabolic syndrome are identified earlier, even if they drink socially, ensuring they receive the necessary metabolic support.
Treatment Options and Lifestyle Reversal
For a long time, the only prescription for fatty liver was weight loss. While this remains the cornerstone of management, the landscape shifted dramatically in recent years. The FDA's approval of resmetirom (Rezdiffra) marked a turning point for patients with moderate to advanced fibrosis. Clinical trials showed this medication helped 26% of patients improve their fibrosis stage compared to 10% of those on a placebo. Before this approval, doctors had to rely on off-label use of other drugs or strict lifestyle modification alone.
However, medication works best when combined with behavior change. Research consistently highlights the impact of weight loss on disease regression. Patients who lose between 7% and 10% of their total body weight often see their NASH regress to simple fatty liver. Even losing just 3-5% can reduce liver fat significantly. This is achievable through dietary changes, increasing physical activity, and managing sleep apnea, which affects 30-50% of those with the condition.
Clinicians also manage associated risks aggressively. Since cardiovascular disease is the leading cause of death in these patients, managing cholesterol, blood pressure, and glucose levels is just as important as treating the liver itself. A holistic approach ensures you protect your heart while healing your liver.

Patient Experiences and Real-World Challenges
Despite advances, the patient journey is rarely straightforward. Many individuals discover they have fatty liver incidentally during blood work for unrelated issues. Community forums reveal frequent stories of diagnostic delays, with nearly half of patients waiting over six months between abnormal results and seeing a specialist. This lag can allow silent fibrosis to progress.
Furthermore, anxiety plays a role. Up to 30% of diagnoses made by non-invasive testing might not be confirmed by biopsy, leading some experts to caution against over-diagnosis and unnecessary worry. Conversely, missing the diagnosis until cirrhosis appears carries severe consequences. Finding a balanced path means knowing your numbers-your FIB-4 score and liver enzyme trends-so you can advocate for timely FibroScans without demanding invasive procedures prematurely.
Success stories often center on patience and consistency. One patient shared their experience of normalizing liver enzymes within two years by prioritizing whole foods and regular movement. Another noted that simply resolving their sleep apnea improved their liver fat percentage noticeably. These anecdotes reinforce that the condition is manageable, provided you stay engaged with your care plan.
Frequently Asked Questions
What is the main difference between NAFLD and NASH?
The primary difference lies in inflammation. NAFLD (or MASLD) encompasses simple fat accumulation without cell damage. NASH (or MASH) includes fat plus inflammation and liver cell injury, which significantly increases the risk of fibrosis and cirrhosis.
How is liver fibrosis measured accurately?
Doctors use blood markers like the FIB-4 score, imaging via FibroScan (measuring stiffness), and sometimes MRI-PDFF to quantify fat. Liver biopsy remains the gold standard for definitive staging but is invasive.
Can I reverse a fatty liver diagnosis naturally?
Yes. Achieving a weight loss of 7-10% of your total body weight can lead to significant improvement, often regressing NASH back to simple fatty liver and reducing fat content.
Are there medications available for NASH in 2026?
Yes. Resmetirom (Rezdiffra) was approved for patients with moderate to advanced fibrosis. Other agents are also in development, though lifestyle changes remain the foundation of therapy.
Why did the name change from NAFLD to MASLD?
The terminology changed to focus on metabolic dysfunction rather than alcohol consumption. This reduces stigma and includes patients who might consume small amounts of alcohol but still suffer from metabolic liver disease.
Rod Farren
April 1, 2026 AT 06:57The distinction between steatosis and steatohepatitis hinges heavily on hepatocyte ballooning presence. Clinicians must utilize transient elastography readings above seven kilopascals to identify significant fibrosis risk factors accurately. Non-invasive markers like APRI and FIB-4 remain standard initial screening tools before considering invasive biopsy procedures. Recent guidelines suggest MRI-PDFF quantification offers superior sensitivity for detecting hepatic fat fraction percentages greater than five percent thresholds. Resmetirom efficacy depends largely on baseline metabolic dysfunction profiles rather than simple lipid accumulation metrics alone. Patients presenting with ALT elevations exceeding fifty units per liter require immediate risk stratification protocols implementation. Understanding the transition from MASLD to MASH involves recognizing inflammatory cytokine activation pathways within the hepatic microenvironment. Fibrosis staging correlates directly with cardiovascular mortality rates independent of liver-related complications severity. Metabolic syndrome components including hypertension significantly accelerate progression toward decompensated cirrhosis phases eventually. Early intervention strategies focusing on caloric restriction show regression potential in non-cirrhotic stages primarily. Monitoring sleep apnea compliance remains crucial for maintaining insulin sensitivity levels throughout the therapeutic duration. Pharmacological agents targeting thyroid hormone receptor beta isoforms demonstrate histological improvement in randomized controlled trials consistently. Clinical management plans should prioritize cardiovascular risk reduction alongside direct hepatoprotective measures simultaneously. Biopsy remains the gold standard despite low complication rates for definitive diagnosis confirmation purposes. Multidisciplinary team approaches yield better long-term outcomes compared to isolated endocrinology referrals traditionally. Strict adherence to these protocols ensures optimal hepatic recovery outcomes in most cases.
Rocky Pabillore
April 2, 2026 AT 14:39While you demonstrate impressive knowledge of technical diagnostics here, most readers simply want practical advice. Your usage of pharmacokinetic terms likely obscures the message for average individuals seeking help. Perhaps simplifying these concepts would serve the community better than listing trial statistics. It is amusing how experts enjoy overwhelming patients with dense academic language constantly.
Owen Barnes
April 4, 2026 AT 01:24i seen alot of ppl here talking bout the fibroscan results. dont trust the numbers blind tho. sometimes it gets off if u r bloated or drank coffee recent. my doc said i had stage 2 scarring but turned out false pos later on. still good to keep track of it though. weight loss works best honestly.
Julian Soro
April 4, 2026 AT 14:19You are taking exactly the right steps by verifying those test results yourself! Doubting initial scans is smart because interference from meals affects accuracy significantly. Your proactive attitude will pay off greatly in managing your long term health. Stay focused on the healthy habits you are building daily!
Christopher Beeson
April 6, 2026 AT 01:41The inevitable decay of cellular integrity mirrors the entropy found in all organic systems ultimately leading to cessation of function without external regulation.
Russel Sarong
April 7, 2026 AT 02:29It is truly terrifying how fast the body breaks down!!! We often ignore the warnings until collapse happens!!! The entropy concept you mention is deeply accurate unfortunately!!! Fighting it requires constant vigilance against our own biology!!! No one wants to face the final breakdown of organ function!!!
Cara Duncan
April 8, 2026 AT 22:44The new terminology finally makes sense to me 🙂🥰
Jenny Gardner
April 9, 2026 AT 04:49The semantic adjustment reflects deeper understanding of pathogenesis! Patients previously excluded due to alcohol history are now correctly identified clinically! This inclusive approach reduces delays in accessing specialized care pathways efficiently! Terminology impacts how insurance companies classify coverage for necessary screenings! We observe improved engagement when language does not carry historical stigma attached! Academic consensus supports shifting focus from abstinence to metabolic health parameters! Public perception shifts positively when educational materials remove judgmental phrasing entirely! Consistency in naming aids research data collection across multiple hospital networks! It enables clearer communication between specialists and general practitioners universally! Such linguistic precision ensures resources are allocated to those with highest risk profiles! Regulatory bodies must adopt these definitions in official coding manuals soon! Health literacy improves significantly when explanations avoid unnecessary negative connotations! Community outreach programs rely on clear terms to engage diverse demographic groups! Stigma removal leads to higher reporting rates of early symptoms by anxious patients! Longitudinal studies benefit from standardized nomenclature throughout their entire duration! Medical journals publish findings using the new acronyms to maintain scientific accuracy!